Pre-Writing Word Budget
Introduction
Healthcare organizations face a threat environment unlike any other industry.
According to IBM's 2025 Cost of a Data Breach Report, healthcare remained the most expensive sector for data breaches, averaging $7.42 million per incident and 279 days to identify and contain. The HHS OCR 2024 Breach Report recorded 663 large breaches affecting nearly 243 million individuals — with hacking and IT incidents accounting for 81% of those reports.
An untested incident response plan doesn't just create compliance exposure. It deepens patient harm, multiplies regulatory liability, and erodes the trust your organization can't afford to lose.
This guide covers:
- HIPAA's specific cyber incident response requirements under the Security Rule
- Breach notification timelines, thresholds, and covered-entity obligations
- How to build a compliant six-phase response plan
- Documentation and forensic evidence obligations
- How NIST SP 800-61 maps to HIPAA's administrative safeguards
Key Takeaways
- HIPAA's Security Rule (§164.308(a)(6)) requires all covered entities and business associates to identify, respond to, mitigate, and document security incidents — size is no exemption
- Not every incident is a notifiable breach; a four-factor risk assessment determines whether formal notification is required
- Large breaches (500+ individuals) require notification to individuals, HHS OCR, and media within 60 calendar days
- A six-phase incident response lifecycle — Preparation through Post-Incident Review — structures how organizations meet HIPAA compliance in practice
- NIST SP 800-61 Rev. 3 is the technical framework HHS references for meeting Security Rule requirements
What Counts as a HIPAA Cyber Security Incident?
The Regulatory Definition
Under 45 CFR §164.304, the HIPAA Security Rule defines a security incident as:
"The attempted or successful unauthorized access, use, disclosure, modification, or destruction of information or interference with system operations in an information system."
Notice that "attempted" is not a qualifier — it's a trigger. Failed ransomware deployments, blocked phishing emails that still reached inboxes, and port scans that never resulted in actual access all qualify as security incidents and activate your response obligations.
Incident vs. Breach: A Critical Distinction
These two terms carry different legal weight, and treating them as equivalent is one of the most common HIPAA compliance mistakes.
| Term | Definition | Triggers |
|---|---|---|
| Security Incident | Any attempted or successful unauthorized access or interference | Incident response procedures |
| Breach | Impermissible acquisition, access, use, or disclosure of unsecured PHI that compromises its security or privacy | Formal breach notification to HHS, patients, and media |
Every breach begins as a security incident, but not every security incident becomes a notifiable breach. A four-factor risk assessment determines which category applies — and that classification directly shapes your notification timeline and legal exposure.
Common Cyber Incidents That Trigger HIPAA Response
The 2024 OCR data identifies the most prevalent incident types in healthcare:
- Ransomware attacks that lock ePHI systems — HHS has explicitly confirmed these constitute security incidents requiring response
- Phishing-driven credential theft — unauthorized access and disclosure drove 94% of small-breach reports in the dataset
- Unauthorized insider access to patient records, whether accidental or intentional
- Lost or stolen devices containing unencrypted ePHI
- Business associate breaches — BAs were implicated in 106 large-breach reports, accounting for 85% of all affected individuals
The Core HIPAA Cyber Incident Response Requirements
What §164.308(a)(6) Actually Requires
Incident response obligations live in §164.308(a)(6) of the Security Rule's Administrative Safeguards. This is a Required standard (not an Addressable one), meaning every covered entity and business associate must comply regardless of size, budget, or technical resources.
The three mandatory elements under §164.308(a)(6)(ii):
- Identify and respond to suspected or known security incidents
- Mitigate, to the extent practicable, the harmful effects of known security incidents
- Document security incidents and their outcomes
Assigned Security Responsibility
§164.308(a)(2) requires organizations to designate a Security Officer responsible for developing and implementing incident response policies. In practice, this person:
- Owns the incident response plan and ensures it stays current
- Coordinates response activities across IT, legal, HR, and communications
- Serves as the primary contact for OCR investigations
- Signs off on breach risk assessments and notification decisions
For smaller organizations, the Security Officer role may be combined with other functions, but the designation must be formal and documented.
Business Associate Obligations
Under 45 CFR §164.314, Business Associate Agreements must require BAs to report security incidents (including breaches of unsecured PHI) to the covered entity. The HITECH Act extended direct OCR liability to business associates, meaning HHS can penalize a BA independently without involving the covered entity.
In practice, if your EHR vendor, billing processor, or cloud storage provider experiences a breach, they must notify you — and you retain breach notification obligations to affected individuals even though your systems weren't the ones attacked.
Proposed 2024 HIPAA Security Rule Updates
HHS published a Notice of Proposed Rulemaking in the Federal Register on January 6, 2025, proposing significant Security Rule updates. As of this writing, no final rule has been issued. Key proposals affecting incident response include:
- Required vulnerability scanning and penetration testing on defined schedules
- Written incident response plan testing and revision requirements
- Specific workforce training timelines and content requirements
Organizations should monitor HHS's regulatory initiatives page for finalization updates, as these proposals would substantially expand incident response obligations.
HIPAA Breach Notification Requirements After a Cyber Incident
The Four-Factor Risk Assessment
When a security incident involves unsecured PHI, you must conduct a breach risk assessment before determining whether notification is required. Notification is required unless you can demonstrate low probability of compromise across all four factors:
- Nature and extent of PHI — types of identifiers involved, likelihood of re-identification
- Who accessed or could have accessed the PHI — whether the unauthorized party is likely to re-disclose it
- Whether PHI was actually acquired or viewed — not just potentially accessible
- Extent to which risk has been mitigated — for example, through retrieval of improperly disclosed records
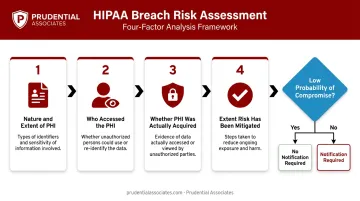
If your assessment cannot affirmatively demonstrate low probability across all four factors, notification is required. Notification is the default; the burden falls on the covered entity to demonstrate otherwise.
Large Breach Notification (500+ Individuals)
For breaches affecting 500 or more individuals, covered entities must notify three parties — all within 60 calendar days of discovering the breach:
- Affected individuals — written notice with specific required content
- HHS OCR — contemporaneous with individual notification
- Prominent media outlets in each affected state or jurisdiction with 500+ residents impacted
Individual notifications must include: what happened, the types of PHI involved, steps affected individuals should take to protect themselves, what the entity is doing to investigate and mitigate, and contact information for questions.
Small Breach Notification (Fewer Than 500 Individuals)
For breaches affecting fewer than 500 individuals:
- Notify affected individuals without unreasonable delay
- Log the breach and submit it to HHS OCR within 60 days after the end of the calendar year in which the breach occurred
Individual notification should not wait for the annual HHS submission. "Without unreasonable delay" applies to affected individuals regardless of breach size.
State Law Overlay
Federal notification rules establish minimums. Several states layer on stricter requirements that may shorten your timeline or expand your reporting obligations:
| State | Key Requirement |
|---|---|
| California | Notice within 30 days of discovery; entities notifying 500+ residents must submit sample notice to AG within 15 days |
| New York | Notice within 30 days; HIPAA-covered entities must notify NY AG within 5 business days of notifying HHS |
| Texas | Breaches affecting 250+ Texans must be reported to the AG within 30 days |
Compliance requires satisfying whichever law is more protective of the individual. Consult legal counsel on applicable state requirements before a breach occurs, not during one.
Penalty Exposure
OCR enforces breach notification violations through a four-tier civil monetary penalty structure tied to culpability level, from unknowing violations to willful neglect uncorrected. The 2025 adjusted annual cap is $2,190,294 per identical violation category — but this cap applies per category, not across all violation types simultaneously, meaning total exposure across multiple violations can be substantially higher.
The Sentara Hospitals $2.175 million settlement illustrates what improper breach reporting costs — OCR reached that agreement after Sentara failed to properly notify HHS of an unsecured PHI breach.
Criminal penalties with potential imprisonment apply to egregious violations.
Building a HIPAA-Compliant Cyber Incident Response Plan
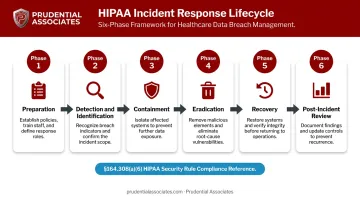
The Six-Phase Lifecycle
A HIPAA-compliant response plan follows a six-phase lifecycle that satisfies §164.308(a)(6) while aligning with established security practice:
- Preparation — designate teams, develop playbooks, test capabilities
- Detection and Identification — monitoring, alerting, initial triage
- Containment — isolate affected systems, stop lateral movement
- Eradication — remove malware, revoke credentials, patch vulnerabilities
- Recovery — restore from verified clean backups, validate system integrity
- Post-Incident Review — root cause analysis, policy updates, lessons learned
Preparation Phase
Effective preparation requires more than having a plan document on file:
- Assign explicit IR team roles: Security Officer, legal counsel, PR/communications lead, and IT forensics lead
- Build scenario-specific playbooks covering ransomware, phishing-driven credential compromise, insider threats, and third-party/BA breaches
- Store all playbooks offline — a plan locked inside an encrypted system is useless during the incident it was meant to address
- Run tabletop exercises at least annually; document reviews alone won't surface coordination gaps
Detection, Containment, and Eradication
Detection requires both automated tooling and human reporting channels:
- SIEM solutions for log aggregation and correlation
- Endpoint Detection and Response (EDR) for real-time endpoint visibility
- Intrusion Detection and Prevention Systems (IDPS) monitoring network traffic
- A clear employee reporting path for suspected incidents — many breaches are first spotted by non-technical staff

Once an incident is identified, containment is the immediate priority. Isolate affected systems from the network before ePHI is further exposed — physical cable removal and controlled network interface isolation are proven containment methods.
With systems contained, eradication can begin: remove malware, revoke compromised credentials, and patch exploited vulnerabilities before any restoration starts.
Recovery and the Contingency Plan Requirement
§164.308(a)(7) requires organizations to maintain a contingency plan that includes a data backup plan, disaster recovery plan, and emergency mode operation plan. Each component is mandatory, and together they form the foundation that makes recovery possible after an incident.
Restoration from backups should proceed only after:
- Forensic acquisition confirms the full scope of the compromise
- Backup integrity is validated (offline backups are the most reliable option)
- All persistence mechanisms are removed and reinfection paths are closed
- All patching and remediation from the eradication phase is complete
When internal teams lack the capacity to execute these steps under time pressure, outside experts with hands-on IR credentials — such as GCIH, GCFA, GREM, and EnCE — can supplement your team without disrupting the forensic chain of custody. Prudential Associates provides that capability for organizations navigating HIPAA-regulated incidents.
Documentation, Forensics, and Post-Incident Review
What HIPAA Requires You to Document
§164.308(a)(6) and §164.316(b) together require organizations to document security incidents and retain that documentation for six years from creation or last effective date. At minimum, each incident record should capture:
- Date and time of discovery
- Nature of the incident and systems affected
- PHI involved (types, volume, affected individuals)
- Who was notified and when
- Containment and eradication actions taken
- Corrective measures implemented
Documentation serves two functions: it satisfies the regulatory retention requirement, and it constitutes your primary defense in an OCR investigation.
The Role of Digital Forensics
Forensic investigation is what transforms an incident into an actionable breach risk assessment. Certified forensic examiners determine:
- Exactly which ePHI was accessed or acquired (critical for the four-factor risk assessment)
- The timeline and scope of unauthorized access
- Whether data exfiltration occurred prior to encryption in ransomware cases
- Root cause and initial attack vector
Examiners must handle evidence under documented chain-of-custody procedures from the moment collection begins. Improper evidence handling can compromise both regulatory investigations and civil litigation. Certifications like EnCE, GCFA, CDFE, and CFCE indicate examiners trained in forensically sound acquisition, the standard OCR and courts expect.
That standard carries real consequences. The April 2025 Northeast Radiology settlement ($350,000) illustrates OCR's focus on failures to review information system activity — specifically audit logs and access reports. Forensic examiners who can reconstruct that activity from preserved evidence are often the difference between a defensible response and a costly enforcement action.
Post-Incident Review
§164.308(a)(8) requires periodic evaluation of security measures — the post-incident review is how that obligation gets met in practice. The review should identify:
- Root cause of the incident
- Gaps in detection or response that allowed the incident to progress
- Required policy or procedure updates
- Workforce training needs
Each finding should produce a concrete remediation task — an updated policy, a new detection rule, or a scheduled training — assigned to a responsible owner with a target completion date.
HIPAA vs. NIST: Aligning Cyber Incident Response Frameworks
NIST SP 800-61 is the technical framework healthcare organizations use to operationalize HIPAA's incident response requirements. Rev. 2 (the classic four-phase framework) was superseded by NIST SP 800-61 Rev. 3 on April 3, 2025, which aligns with the NIST Cybersecurity Framework 2.0.
How NIST phases map to HIPAA requirements:
| NIST SP 800-61 Phase | HIPAA Administrative Safeguard |
|---|---|
| Preparation | §164.308(a)(6)(i) — Implement policies and procedures |
| Detection and Analysis | §164.308(a)(6)(ii) — Identify suspected or known incidents |
| Containment, Eradication & Recovery | §164.308(a)(6)(ii) — Respond and mitigate harmful effects |
| Post-Incident Activity | §164.308(a)(8) — Periodic evaluation |
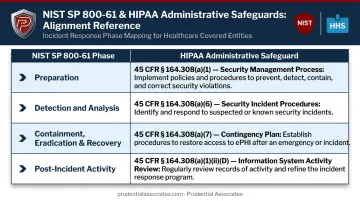
These frameworks work together. HHS's own Health Industry Cybersecurity Practices (HICP) publication explicitly references NIST as implementation guidance for Security Rule compliance — meaning an IR program built on NIST SP 800-61 gives organizations a recognized federal standard to point to when OCR comes asking.
That auditability matters in practice. Prudential Associates structures healthcare incident response engagements around NIST SP 800-61, customized to each client's operations, so the resulting documentation holds up under OCR scrutiny.
Frequently Asked Questions
What are HIPAA's cyber incident response requirements?
HIPAA's Security Rule (§164.308(a)(6)) requires covered entities and business associates to implement policies to identify and respond to security incidents, mitigate their harmful effects, and document all incidents and outcomes. The Breach Notification Rule layers in formal reporting obligations when a risk assessment confirms unsecured PHI was compromised.
Is HIPAA or 42 CFR Part 2 more strict?
42 CFR Part 2, which governs substance use disorder treatment records, is generally more restrictive than HIPAA — particularly around consent requirements for disclosure and limits on using records in legal proceedings against patients. Organizations treating SUD patients must reconcile and comply with both sets of rules.
What is the NIST standard for cyber incident response?
NIST SP 800-61 Rev. 3 (finalized April 2025) is the primary standard, built around NIST Cybersecurity Framework 2.0 functions; its predecessor Rev. 2 defined the four foundational phases: Preparation, Detection and Analysis, Containment/Eradication/Recovery, and Post-Incident Activity. HHS explicitly references NIST frameworks as implementation guidance for HIPAA Security Rule compliance.
What is the difference between a HIPAA security incident and a reportable breach?
A security incident is any attempted or successful unauthorized access to or interference with an information system — it triggers your response process. A breach is a specific subset: an impermissible use or disclosure of unsecured PHI requiring formal notification unless a four-factor risk assessment demonstrates low probability of compromise.
What are the penalties for failing to comply with HIPAA incident response requirements?
OCR civil monetary penalties span four culpability tiers, from unknowing violations to uncorrected willful neglect. The 2025 adjusted annual cap is $2,190,294 per identical violation category, applied per category rather than across all violations simultaneously. Criminal charges with potential imprisonment apply to the most egregious violations.
How long must HIPAA security incident documentation be retained?
Under §164.316(b)(2), all HIPAA documentation — including security incident records — must be retained for a minimum of six years from the date of creation or the date it was last in effect, whichever is later, and must be accessible to persons responsible for implementing the documented procedures.