
Introduction
Healthcare organizations handle some of the most sensitive personal data that exists — medical histories, insurance details, Social Security numbers — and the people most likely to compromise that data already have the keys to the building.
According to the Verizon 2025 Data Breach Investigations Report, internal actors were responsible for 30% of healthcare breaches in 2025 — a figure that, while lower than 2024's striking 70%, still reflects a persistent and structurally unique risk. Unlike external attackers who must break through defenses, insiders operate with legitimate credentials and established access patterns. That's what makes them far harder to detect.
Whether the cause is deliberate data theft or a careless mistake, the consequences are the same: exposed Protected Health Information (PHI), HIPAA penalties reaching into the millions, and lasting damage to patient trust. For healthcare organizations, early detection and systematic prevention are baseline requirements — not optional additions to a security program.
Key Takeaways
- Healthcare insiders include employees, contractors, business associates, and former staff with legitimate system access
- 30% of 2025 healthcare breaches involved internal actors, per Verizon's DBIR
- Insider threats evade perimeter defenses because the access is authorized — detection requires behavioral monitoring
- Prevention requires layered controls: access governance, MFA, DLP, training, and formal offboarding
- Suspected incidents require structured forensic investigation before any disciplinary or legal action
Types of Healthcare Insider Threats
The term "insider" extends well beyond current employees. Contractors, business associates, researchers, volunteers, and former staff with active credentials all represent potential insider risk — anyone with authorized access to systems containing PHI qualifies.
Malicious Insider Threats
Deliberate insider actions typically fall into a few recognizable patterns:
- PHI theft for financial gain — selling patient records to identity theft rings or on dark web markets
- Intellectual property theft — exfiltrating research data or proprietary clinical protocols
- Credential sharing — selling login access to external actors
- Sabotage — disrupting clinical systems before departure
The Montefiore Medical Center case shows what these threats cost in practice. HHS OCR's settlement agreement documents an employee who stole and sold ePHI belonging to 12,517 patients to an identity theft ring — resulting in a $4.75 million settlement and OCR findings of audit control failures.
Non-Malicious Insider Threats
Not every insider breach involves bad intent. Negligent and accidental actions are just as prevalent — and statistically, more frequent:
- Accessing a celebrity patient's records out of curiosity
- Sending PHI to the wrong email recipient
- Clicking a phishing link and handing over credentials
- Leaving a workstation unattended and unlocked
- Informally sharing login credentials with a colleague
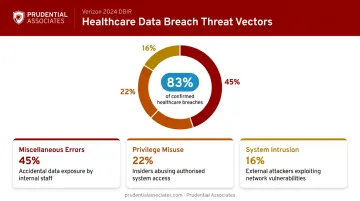
According to the Verizon 2024 DBIR Healthcare Snapshot, Miscellaneous Errors, Privilege Misuse, and System Intrusion together accounted for 83% of confirmed healthcare breaches — with Miscellaneous Errors ranking first.
From a HIPAA standpoint, intent is irrelevant. A misdirected fax containing PHI carries the same notification obligations as deliberate theft.
Consequences of Unchecked Insider Threats
Regulatory and Financial Exposure
HIPAA civil monetary penalties are significant and tiered by culpability. Under the 2026 inflation-adjusted figures, penalties range from $145 per violation (no knowledge) to $2,190,294 per violation (willful neglect, uncorrected), with annual caps at the same maximum figure.
Beyond fines, organizations face mandatory breach notification — affected individuals must be notified within 60 calendar days of discovery, HHS must be notified for breaches affecting 500 or more individuals within the same window, and media notification is required when 500 or more residents of a state are affected.
Insider breaches compound liability because they tend to go undetected far longer than external attacks. IBM's 2025 Cost of a Data Breach Report places healthcare's average breach cost at $7.42 million — the highest of any industry — with an average lifecycle of 279 days to identify and contain.
Operational and Reputational Damage
The financial penalties extend well beyond fines. Organizations also face:
- Erosion of patient confidence that directly affects retention
- Increased cyber insurance premiums following a reported breach
- Civil litigation from affected patients
- Operational disruption during forensic investigation and remediation
The 2025 BayCare Health System settlement ($800,000) stemmed from a former non-clinical staff member using active credentials to access a patient's ePHI after separation. OCR cited failures in access authorization and activity review — a reminder that unrevoked credentials remain exploitable long after an employee departs.
Warning Signs of an Emerging Insider Threat
Understanding these consequences makes early detection a business imperative, not just a compliance checkbox. These are the signals worth monitoring.
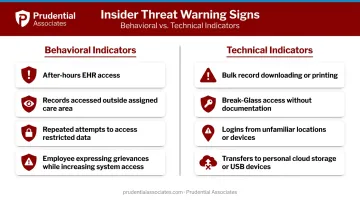
Behavioral indicators to watch:
- After-hours EHR access with no on-call justification
- Accessing records of patients outside an assigned care area or panel
- Repeated attempts to reach restricted data or systems
- An employee openly expressing grievances or signaling intent to resign while simultaneously increasing data access
Technical indicators to monitor:
- Bulk downloading or printing of patient records in a single session
- Break-Glass access events without matching clinical documentation
- Logins from unfamiliar devices or geographic locations
- Transfers to personal cloud storage or USB devices
How to Detect Healthcare Insider Threats
Detection requires a fundamental shift in mindset. Because insider access is authorized by definition, perimeter security alone cannot catch it. The question isn't whether a user has access — it's what they're doing with it.
Deploy User and Entity Behavior Analytics (UEBA)
UEBA builds behavioral baselines for each user role, device, and service account, then flags statistical deviations from those baselines. In a healthcare context, meaningful signals include:
- A clinician accessing significantly more records than their peer cohort in the same role
- Off-shift login surges inconsistent with historical patterns
- Mass export or print activity across a large patient population
- Break-Glass invocations that don't correlate with any documented clinical event
UEBA becomes most effective through integration. Feeding UEBA signals into a SIEM enables cross-source correlation that no single data stream can replicate. Relevant sources include:
- EHR audit logs and directory authentication events
- VPN records and badge swipe data
- EDR telemetry and DLP alerts
Together, these inputs surface patterns that isolated monitoring consistently misses.
HIPAA's Security Rule (45 CFR 164.308 and 164.312) requires both audit controls and regular review of system activity records. UEBA directly supports both obligations at a scale that manual review cannot match.
Implement and Audit PHI Access Logs
HIPAA requires healthcare organizations to implement mechanisms that record and examine activity in systems containing ePHI. Across large EHR environments, manual review cannot keep pace — automated alerting is how organizations meet this obligation in practice.
High-risk patterns worth automated alerting:
- A single user accessing 100+ patient records in one session
- Access to VIP, deceased, or terminated patient records
- Repeated access to records with no treating relationship
Automated alerts should be supplemented by periodic manual audits of high-privilege accounts, where the volume of access may be legitimately high but the pattern still warrants review.
Leverage Digital Forensics When Threats Are Suspected
Behavioral signals flag risk; they don't establish guilt. When monitoring surfaces a credible insider threat, a formal digital forensic investigation is required to:
- Preserve evidence in a forensically sound manner
- Establish and maintain chain of custody
- Determine the full scope and timeline of unauthorized access
- Produce findings admissible in disciplinary proceedings, litigation, or regulatory review

Organizations without in-house forensic capability should engage a certified external investigator before taking any disciplinary or legal action. Acting prematurely — without preserved, chain-of-custody evidence — can undermine both internal proceedings and any subsequent OCR or legal process.
Prudential Associates combines cybersecurity expertise with law enforcement investigative discipline. Their examiners perform forensically sound acquisitions using write blocking, validated imaging methods, and cryptographic hashing — with every step documented for defensibility. CEO Jared Stern has testified as a digital forensics expert in state and federal courts more than 500 times, a depth of courtroom experience that matters when insider incidents escalate to litigation or OCR proceedings.
Best Practices for Healthcare Insider Threat Prevention
Prevention is layered. No single control is sufficient — effective programs address people, process, and technology simultaneously.
Enforce Least Privilege and RBAC
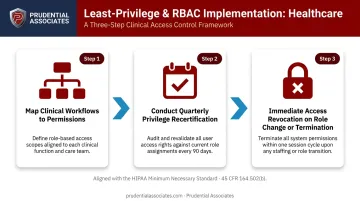
Map clinical workflows to permissions and assign Role-Based Access Control (RBAC) so each user accesses only the PHI required for their role. HHS ties this directly to HIPAA's Minimum Necessary standard under 45 CFR 164.502(b).
- Eliminate broad "power user" accounts wherever possible
- Conduct quarterly privilege recertification reviews
- Revoke access immediately on role change or termination — not at the end of the pay period
This limits the blast radius of any compromised or rogue account. Lateral movement is contained even when credentials are stolen. Combining least privilege with strong authentication reinforces this containment further.
Require Multi-Factor Authentication
Enforce MFA for remote access, privileged workflows, and EHR access. HHS 405(d) HICP lists Access Management — including MFA — among its 10 core healthcare cybersecurity practices.
Key implementation points:
- Prohibit shared accounts and generic clinical logins
- Enforce strong password policy technically, not just in writing
- Extend MFA to all clinical application access as a near-term priority
With authentication hardened, the next control layer addresses what happens when data moves — intentionally or otherwise.
Deploy Data Loss Prevention and Endpoint Controls
DLP tools inspect and can block unauthorized PHI transfers across email, cloud uploads, USB devices, and print jobs. HHS 405(d) HICP specifically lists Data Loss Prevention as a recommended healthcare cybersecurity practice.
Pair DLP with:
- PHI encryption at rest and in transit
- Full-disk encryption on all portable devices
- DLP policies tuned to clinical workflows to avoid impeding legitimate care coordination
Endpoint controls ensure that device loss or theft doesn't automatically become a reportable breach.
Conduct Role-Specific Security Awareness Training
Most negligent insider incidents stem from a lack of awareness, not bad intent. Training should be:
- Tailored by role — clinicians, administrative staff, and IT personnel face different threats
- Built around scenarios — phishing simulations produce more durable learning than slide decks
- Delivered repeatedly — annually at minimum, and after relevant policy changes
- Covering HIPAA Privacy and Security Rules, PHI handling, acceptable EHR use, and anonymous reporting channels for suspicious colleague behavior
Complete training before granting PHI access at onboarding — not after.
Establish Formal Offboarding and JML Processes
Former employees and contractors retaining active credentials after departure is a well-documented attack vector — the BayCare Health System settlement, which resulted from an employee accessing patient records post-termination, illustrates how costly this gap can be.
Automation closes this gap reliably:
- Integrate HR termination workflows with identity management systems
- Make access revocation simultaneous with employment termination — not a manual step completed days later
- Extend the same process to contractors and business associates
- Document and audit every offboarding action
Long-Term Insider Threat Management Strategies
Detection controls and prevention policies require ongoing investment to remain effective. Insider threats evolve — both in sophistication and in the people who pose them.
Key long-term practices:
- Run tabletop exercises and red team simulations at least annually to test incident response playbooks, detection capabilities, and staff readiness against realistic insider scenarios
- Adopt Zero Trust architecture by shifting from network-perimeter trust to continuous verification of every access request — using identity, device posture, and behavioral context (per CISA's Zero Trust Maturity Model 2.0; NIST SP 800-66 Rev. 2 specifically links zero trust principles to ePHI access control)
- Build a formal Insider Threat Program (ITP) with cross-functional ownership across IT security, HR, legal, and privacy; document and consistently enforce a sanctions policy communicated to all staff (CISA's insider threat mitigation frameworks are a practical starting point)
- Engage a Managed Detection and Response (MDR) provider if 24/7 in-house security operations aren't feasible — continuous monitoring of insider risk signals without requiring additional headcount

Prudential Associates offers MDR capabilities backed by over 50 years of operational experience and an international network of security specialists. Their certified analysts correlate behavioral signals across endpoints, networks, and cloud environments, applying the investigative judgment that purely automated tools miss.
Conclusion
Healthcare insider threats — deliberate or accidental — are not inevitable. They're identifiable, detectable, and preventable when organizations commit to a program that combines access governance, behavioral monitoring, workforce training, and a tested incident response plan.
Proactive investment in insider threat detection costs a fraction of what follows an undetected breach. Organizations that treat insider risk as an ongoing program — not a one-time policy exercise — avoid the worst outcomes:
- HIPAA fines and OCR investigations
- Patient notification obligations and associated costs
- Litigation exposure from affected individuals
- Reputational damage that erodes patient trust
When an incident does occur, having certified forensic investigators involved early makes the difference between a contained event and a prolonged crisis. Prudential Associates' insider threat investigation practice supports healthcare organizations through every stage — from behavioral anomaly analysis to legally defensible evidence collection and incident reporting.
Frequently Asked Questions
How do you detect an insider threat?
Detection relies on monitoring what authorized users do with their access, not just whether they have it. Tools like UEBA and SIEM analyze behavioral baselines and flag anomalies — unusual access volume, off-hours activity, bulk data transfers — while regular audit log reviews surface patterns that automated tools may miss.
What are recommended practices for mitigating insider threats?
Core mitigation layers include:
- Least-privilege access with RBAC and MFA on all remote and privileged accounts
- DLP controls governing PHI movement and ongoing HIPAA security awareness training
- Formal offboarding that revokes access simultaneously with employment termination, not days later
What ensures PHI included in an email remains secure?
PHI sent by email requires end-to-end encryption, a HIPAA-compliant platform with a signed Business Associate Agreement, and DLP controls that intercept misdirected messages before delivery. Employee training on verifying recipient identity is equally critical, since most PHI email incidents stem from human error rather than technical failure.
What is the difference between a malicious and a non-malicious insider threat in healthcare?
Malicious insiders act deliberately: stealing records for financial gain, selling credentials, or sabotaging systems. Non-malicious insiders cause harm through negligence or curiosity, such as clicking phishing links or snooping on acquaintance records. Both categories carry the same HIPAA liability; intent shapes the enforcement narrative, not the notification obligation.
What are the most common warning signs of an insider threat in a healthcare setting?
Key red flags include accessing patient records outside one's assigned care area, bulk downloading or printing activity, anomalous Break-Glass usage without clinical documentation, login activity from unfamiliar locations or devices, and an employee expressing intent to resign while simultaneously increasing data access patterns.
How does HIPAA require healthcare organizations to respond to insider breaches?
HIPAA requires a four-factor risk assessment under 45 CFR 164.402 to determine whether a reportable breach occurred. If confirmed: affected individuals must be notified within 60 days; HHS must be notified for breaches affecting 500 or more individuals; media notification applies when 500 or more state residents are affected. A documented sanctions policy must also be applied consistently.


